


FILE – This Oct. 14, 2015, file photo shows the Food and Drug Administration campus in Silver Spring, Md. (Photo: AP)
I routinely grouse about the heavy economic cost of red tape. I’ve also highlighted agencies (such as the EEOC) that seem especially prone to senseless regulations.
And I’ve explained why private regulation actually is a very effective way of promoting health and safety.
Today, let’s get specific and look at the Food and Drug Administration. This bureaucracy ostensibly is supposed to protect us by making sure drugs and medical devices are safe and effective before getting approval, which seems like it might be a reasonable role for government.
But the FDA routinely does really foolish things that undermine public health. The likely reason is that the bureaucracy has a bad incentive structure. As Professor Alex Tabarrok has explained.
…the FDA has an incentive to delay the introduction of new drugs because approving a bad drug (Type I error) has more severe consequences for the FDA than does failing to approve a good drug (Type II error). In the former case at least some victims are identifiable and the New York Times writes stories about them and how they died because the FDA failed. In the latter case, when the FDA fails to approve a good drug, people die but the bodies are buried in an invisible graveyard.
This video from Learn Liberty looks at some data on how the FDA’s Type II errors have led to thousands of deaths, but mostly focuses on whether people and medical professionals should have the freedom to makes choices different from what the FDA has officially blessed.
It’s also worth mentioning that the process of drug approval is jaw-droppingly expensive, as Professor Tabarrok noted in another column.
It costs well over a billion dollars to get the average new drug approved and much of that cost comes from FDA required clinical trials. Longer and larger clinical trials mean that the drugs that are eventually approved are safer. But longer trials also mean that good drugs are delayed. And the more expensive it is to produce new drugs the fewer new drugs will be produced. In short, longer and larger trials mean drug delay and drug loss.
The FDA bureaucracy can’t even approve things it already has approved. There was a big controversy a few months ago about the EpiPen, which is a very expensive device that auto-injects medication to people suffering severe allergic reactions.
But the device is only costly because the FDA is hindering competition, as noted by the Wall Street Journal.
Epinephrine is a basic and super-cheap medicine, and the EpiPen auto-injector device has been around since the 1970s. Thus EpiPen should be open to generic competition, which cuts prices dramatically for most other old medicines. Competitors have been trying for years to challenge Mylan’s EpiPen franchise with low-cost alternatives—only to become entangled in the Food and Drug Administration’s regulatory afflatus. …the FDA maintains no clear and consistent principles for generic drug-delivery devices like auto injectors or asthma inhalers. …injecting a kid in anaphylactic shock with epinephrine…is not complex medical engineering. But no company has been able to do so to the FDA’s satisfaction.
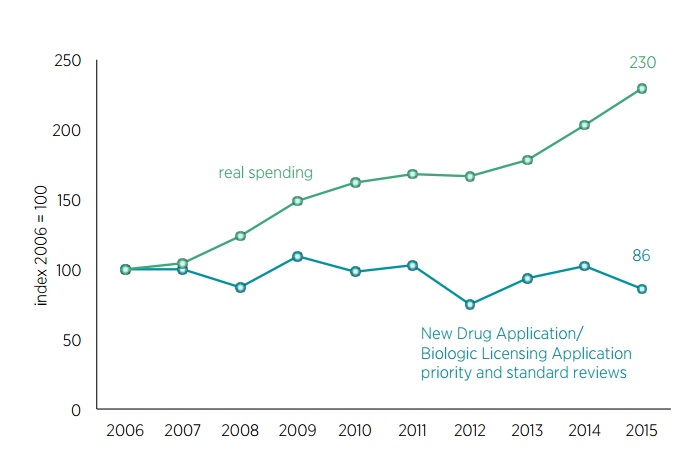
Research from the Mercatus Center reveals that the FDA imposes ever-higher costs and gets ever-higher budgets, but also how the bureaucracy fails to deliver on its obligation to facilitate innovation.
The expense of putting drugs and devices through this system is almost unimaginable. The cost of bringing low- to medium-risk 510(k) medical devices to market averages $31 million, $24 million (75 percent) of which is dedicated solely to attaining FDA approval within an average of about six months. Any significant improvement to the device requires reapplication. For higher-risk medical devices where there may be significant health gains, the costs are about $94 million, $75 million (80 percent) of which is dedicated to attaining FDA approval. For drugs, the situation is much worse.
It costs an average of $2.6 billion simply to get a drug through the FDA process and onto the market. This does not include postmarket monitoring, the terms of which are laid out by FDA upon approval. These costs have increased from about $1 billion between 1983 and 1994. …we continue to increase the funding and authority for FDA and assume that we will somehow boost innovation in medical products (drugs and devices) despite the growing obstacles. This has not happened. …Congress continues to increase funding for FDA through both the general fund and industry user fees…with the hope that performance goals and additional funding would increase FDA’s performance and lead to an increase in innovations. …but FDA finds strategic ways to narrowly meet each goal while frustrating the original goal of improving health outcomes through innovation.
By the way, the FDA also does really bone-headed things. I’ve previously written about the bureaucracy’s war against unpasteurized milk, including military-style raids on dairies. Now the bureaucrats think soldiers shouldn’t be allowed to get cigars.
The Wall Street Journal has the details of this silly nanny-state intervention.
You might think GIs in Iraq and Afghanistan have enough to worry about with Islamic State and the Taliban. But it turns out they’ve also got a problem called the Food and Drug Administration. In August a new FDA rule went into effect that forbids tobacco makers and distributors from handing out free samples. Some companies that have been donating cigars to service members for decades have now stopped for fear that this is now illegal. The FDA nuttiness has attracted the attention of Rep. Kathy Castor, a Democrat who represents Florida’s 14th district, which includes “Cigar City,” or Tampa. She has introduced a bill to “reinstate the tradition of donating cigars to our military members to provide them with a taste of home while deployed.” Her press release notes that cigars are the “second-most requested item” from troops overseas. …cigars for service members is in question because it’s a proxy for the political war on tobacco, but the first casualty is common sense. The FDA’s bureaucrats are happy to have U.S. soldiers, sailors, airmen and Marines dodge bullets overseas but they’re horrified they might relax by lighting up a stogie.
But the nanny-state war against soldiers enjoying cigars is downright trivial compared to the deadly impact of the FDA’s attack on vaping.
Jacob Sullum of Reason outlines some of the horrifying details.
The Food and Drug Administration’s e-cigarette regulations, which took effect last week, immediately struck two blows against public health. As of Monday, companies that sell vaping equipment and the fluids that fill them are forbidden to share potentially lifesaving information about those products with their customers. They are also forbidden to make their products safer, more convenient, or more pleasant to use. The FDA’s censorship and its ban on innovation will discourage smokers from switching to vaping, even though that switch would dramatically reduce the health risks they face. That effect will be compounded by the FDA’s requirement that manufacturers obtain its approval for any vaping products they want to keep on the market for longer than two years. The cost of meeting that requirement will force many companies out of business… All of this is unambiguously bad for consumers and bad for public health. Yet the FDA took none of it into account…the Family Smoking Prevention and Tobacco Control Act…gave the FDA authority over tobacco products, a category to which it has arbitrarily assigned tobacco-free e-cigarettes, even when they contain nicotine that is not derived from tobacco or no nicotine at all. …A brief that 16 advocates of tobacco harm reduction filed last week in support of Nicopure’s lawsuit notes that the cost of the FDA’s regulations will far outweigh their benefit if they cause even a small percentage of vapers to start smoking again or deter even a small percentage of current smokers from switching. That’s because of the huge difference in risk between e-cigarettes and the conventional kind (at least 95 percent, according to the Royal College of Physicians)… The FDA acknowledges that its regulations might also harm public health by retarding the substitution of vaping for smoking. But it does not include that cost in its analysis, deeming it too speculative. The FDA literally assigns zero value to the lives of smokers who would have quit were it not for the agency’s heavy-handed meddling.
Oh, I suppose I also should mention that FDA red tape is responsible for the fact that Americans have a much more limited selection of condoms than Europeans.
I’m sure there’s a good joke to be made about the bureaucrats screwing us in ways that interfere with us…um…well, you know.
Let’s wrap up with some tiny bits of good news. First, Arizona’s Goldwater Institute has been remarkably successful in getting states to adopt “Right to Try” laws that give seriously ill people the right to try investigational medications.
Sadly, those laws will have limited use until there’s also reform in Washington. Fortunately, there’s some movement. Here’s a video from a congressional hearing organized by Senator Johnson of Wisconsin.
Here’s a second item that sort of counts as good news.
If there is one silver lining to the dark cloud of FDA incompetence, it’s that the bureaucrats haven’t figured out how to criminalize those who use drugs for “off-label” purposes (i.e., for reasons other than what was approved by the government). A good example, as reported by the New York Times, is a tooth desnsitizer that’s only been recently approved by the FDA (after being available for decades in nations such as Japan), and already dentists are using it to fight cavities.
Nobody looks forward to having a cavity drilled and filled by a dentist. Now there’s an alternative: an antimicrobial liquid that can be brushed on cavities to stop tooth decay — painlessly. The liquid is called silver diamine fluoride, or S.D.F. It’s been used for decades in Japan, but it’s been available in the United States, under the brand name Advantage Arrest, for just about a year. The Food and Drug Administration cleared silver diamine fluoride for use as a tooth desensitizer for adults 21 and older. But studies show it can halt the progression of cavities and prevent them, and dentists are increasingly using it off-label for those purposes. …Silver diamine fluoride is already used in hundreds of dental offices. Medicaid patients in Oregon are receiving the treatment…it’s relatively inexpensive. …The noninvasive treatment may be ideal for the indigent, nursing home residents and others who have trouble finding care. …But the liquid may be especially useful for children. Nearly a quarter of 2- to 5-year-olds have cavities
Since I’m not familiar with the history of the FDA, I wonder whether the bureaucrats have ever tried to block medical professionals from using drugs and devices for “off-label” purposes.
Let me close with one final point. Our leftist friends aren’t very interested in reforming the FDA.
Instead, they argue that the big problem is greedy pharmaceutical companies and suggest European-style price controls.
That could save consumers money in the short run, I’m sure, but it would gut the incentive to develop new medications.
One expert looked at the Rand Corporation estimates that such policies would lead to a decline in life expectancy of 0.7 years by 2016. He then crunched the numbers and concluded that the aggregate impact would be worse thing to ever happen. Even worse than the brutality of Mao’s China.
…let me put this in context. In 2060 there will probably be 420 million Americans and 523 million Europeans. And suppose that whatever changes we make in drug regulations today last for one human lifespan, so that everybody has a chance to be 55-60. So about a billion people each losing about 0.7 years of their life equals 700 million life-years. Since some people live in countries outside the US and Europe [citation needed] and they also benefit from First-World-invented medications, let’s round this up to about a billion life-years lost. What was the worst thing that ever happened? One strong contender is Mao’s Great Leap Forward, in which ineffective agricultural reforms and very effective purges killed 45 million people. Most of these people were probably already adults, and lifespan in Mao’s China wasn’t too high, so let’s say that each death from the Great Leap Forward cost what would otherwise be twenty healthy life years. In that case, the worst thing that has ever happened until now cost 45 million * 20 = 900 million life-years. Once again, RAND’s calculations plus my own Fermi estimate suggest that prescription drug price regulation would cost one billion life-years, which would very slightly edge out Communist China for the title of Worst Thing Ever.
I guess the bottom line is that the FDA is a typical regulatory agency, both incompetent and expensive. But if the statists have their way, things could get a lot worse.






